


Contamination of Human Blood with Self-Assembling Micro/Nanotechnology in the post-CV19 “Vaccine” era (updated)
Has Your Blood been Adulterated? How can You Know?



Calamari-like “Clot” photos courtesy of Laura Kasner
It has been over three years since the first reports were published in which undeclared constituents were found in CV19 injections. The first detailed report of which I am aware was that of Dr. Pablo Campra [1], who concluded that all of the four major (Pfizer, Moderna, AstraZeneca and J&J) CV19 injectable product brands/trademarks contain significant amounts of graphene which is known to be toxic [2] to humans and animals. [3] A total of 26 teams throughout the world have since conducted tests which document graphene and other toxic and undeclared chemicals in CV19 injectables. [4] Numerous nondisclosed and potentially toxic metals and other elements have been found in a myriad of childhood vaccines. [5]
As early as 2021, microscopists began analyzing the contents of CV19 vaccine vials and subsequently, human blood, after learning that many were adulterated with undisclosed substances and that very few of those examined, contained any significant amount of mRNA, DNA or other organic materials. [6] Some of the earliest reports disclosed stunning images of what appeared to be self-organizing and self-assembling micro and nanotechnology. One example is from the work of Dr. David Nixon who began publishing images and videos of what appeared to be self-assembling nanorobotics in CV19 vial contents. Nixon, in collaboration with Dr. Ana Maria Mihalcea, Shimon Yanowitz, Mateo Taylor, Clifford Carnicom and others tried repeatedly to sound the alarm but were largely met with silence or derision. Since that time, many other investigators have joined in the effort. [7] In addition to human blood, [vaccine contents, a plethora of other injectable substances such as dental anesthetics] [8], insulin and even oral nutritional supplements and medications have been analyzed, many of which show obvious evidence of MT/NT contamination/adulteration.
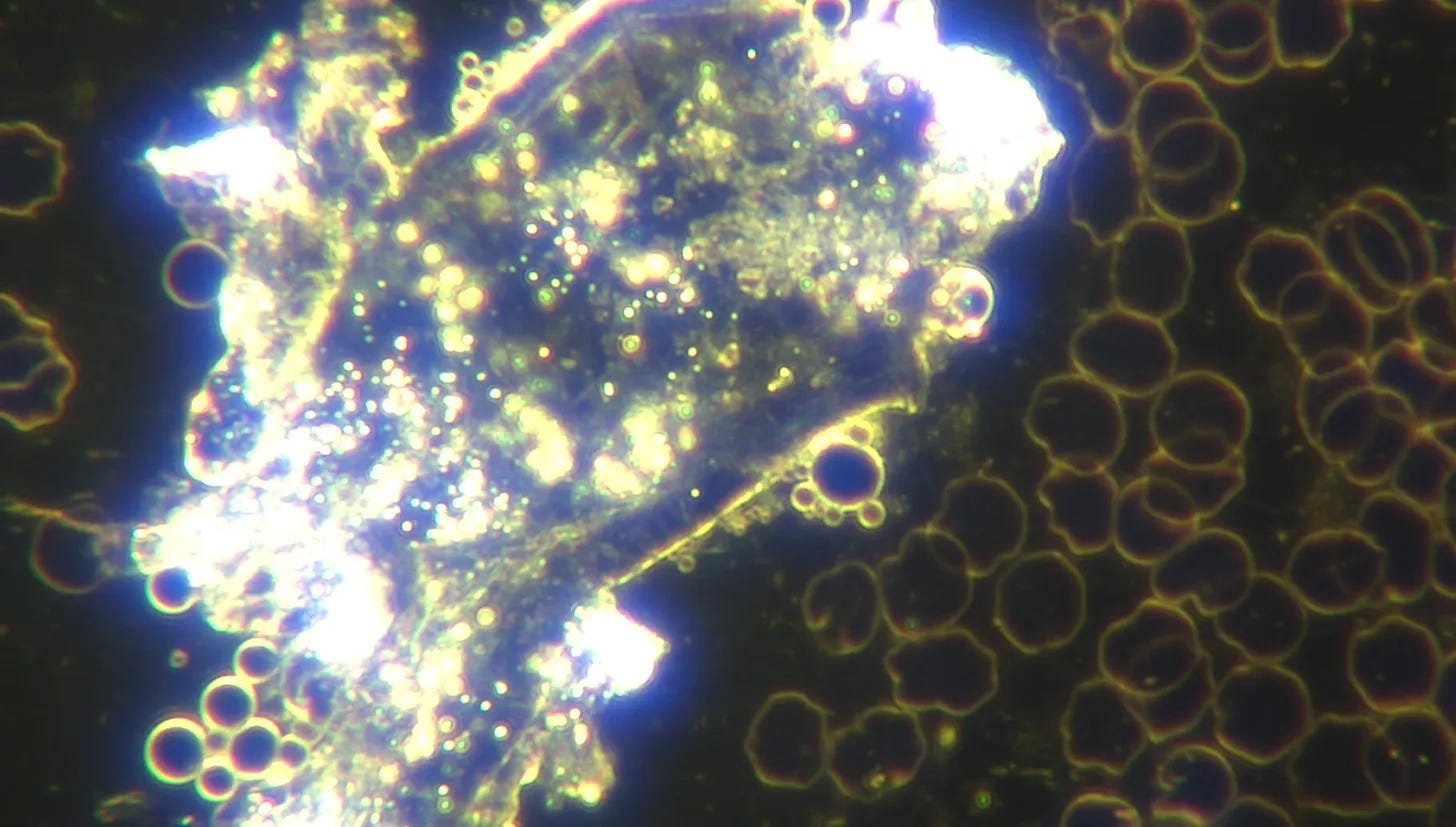
There is now incontrovertible evidence that human blood is contaminated with self-assembling micro/nanotechnology (MT/NT) [9] and that compared with 2021, there is, three years later, a great deal more evidence of it, even in those with no history of CV19 vaccination or PCR swab testing.

Unvaccinated blood with Area of micelles filled with nanorobots, courtesy of Dr. Ana Maria Mihalcea
Hydrogels and Quantum Dots that glow in Multiple Colors, courtesy of Dr. Ana Maria Mihalcea
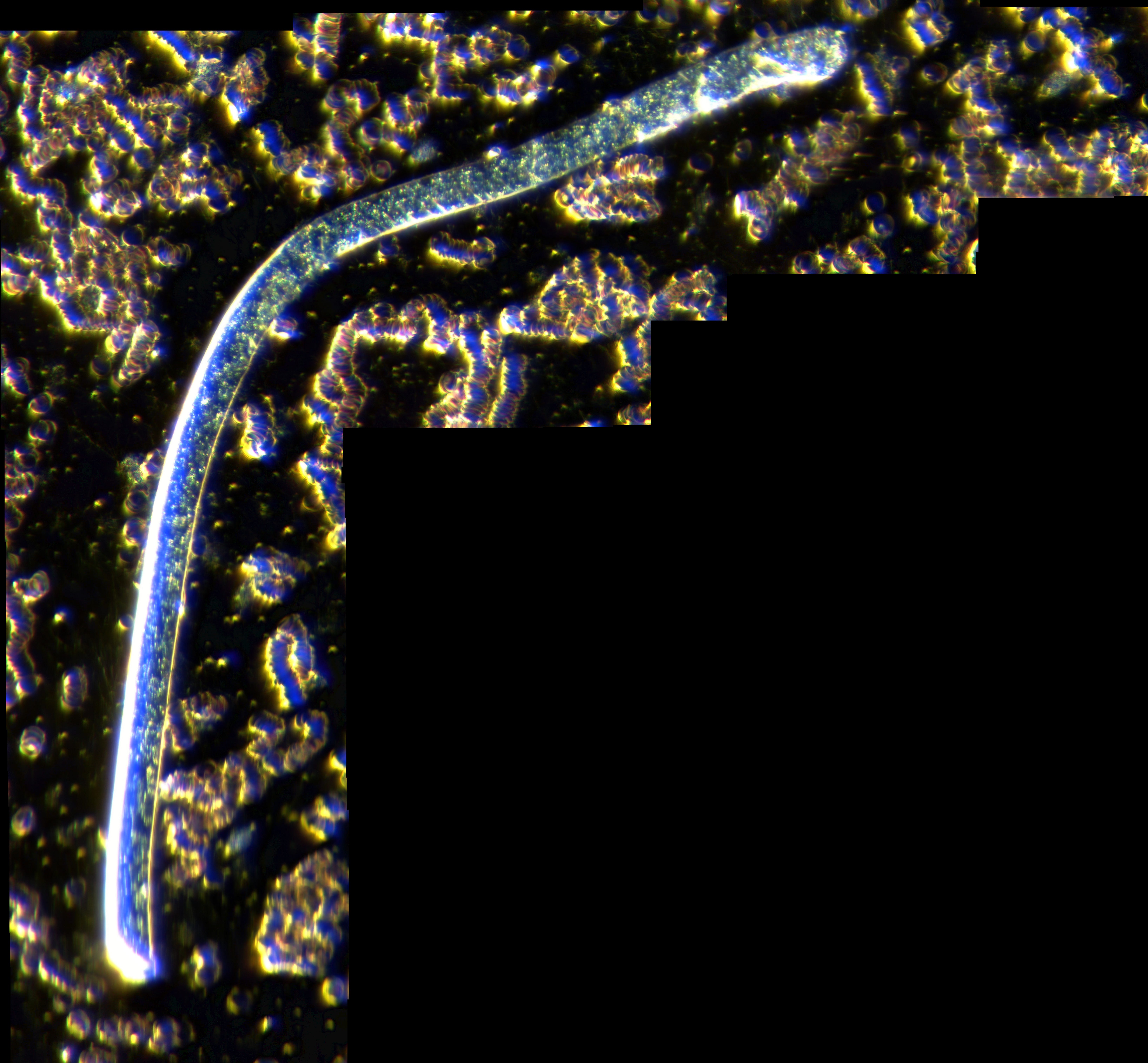

Colored lights in a fiber, in our blood with close-up, courtesy Matt’s Microscopy
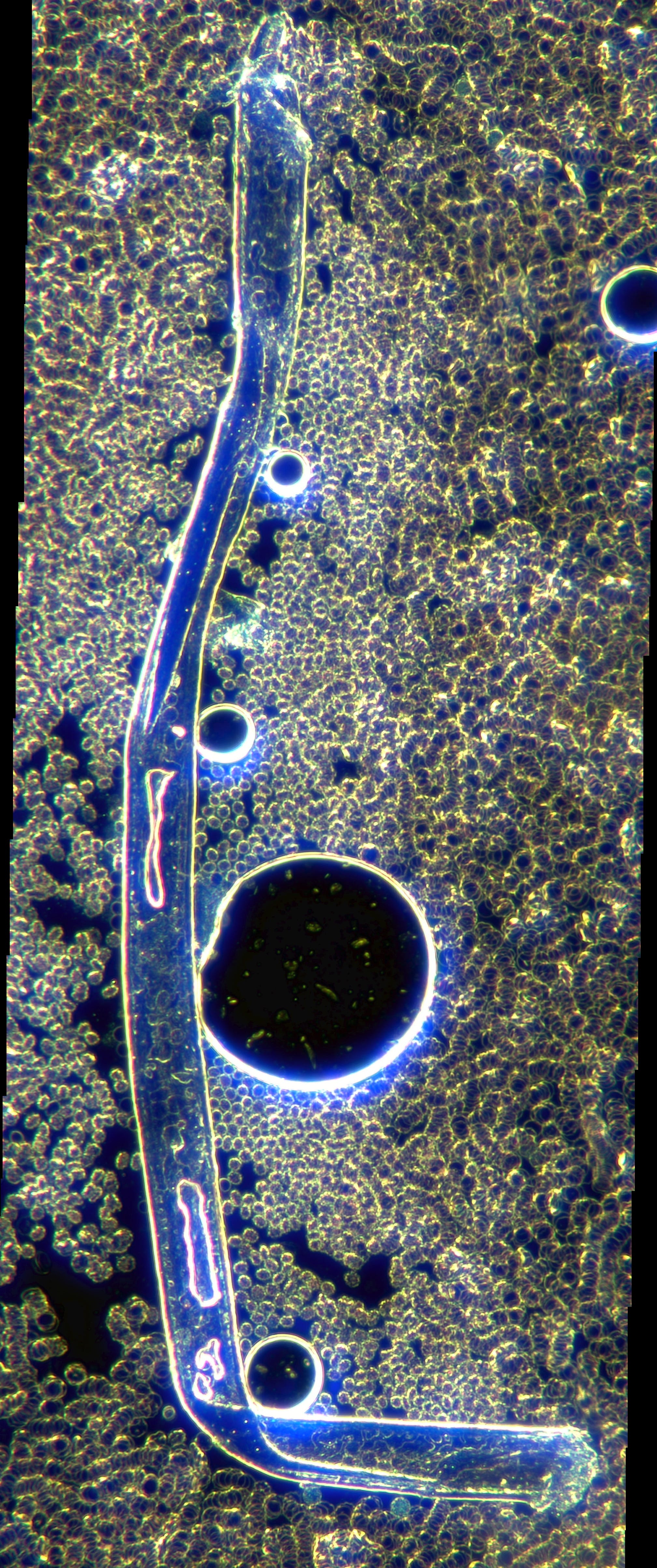
Fibers and Self-Assembly Spheres in Blood, courtesy Matt’s Microscopy
One of the issues that came to mind after watching Dr. Anita Baxas’ May, 2024 Florida presentation entitled; Preliminary Treatment Protocols for the Covid Vaccine Injured [10] and thinking about it more deeply [11], is that there are 2 different subsets of people from the perspective of microtech/nanotech infestation; the [CV19 vaccinated and CV19 unvaccinated] [12] but that may no longer be the critical factor for determining whether a person has significant microtech or nanotech infestation in their body. [13] It may be that a better metric is whether they are symptomatic or not. While the multiply CV19 vaccinated and PCR swabbed, seem to be the most heavily contaminated, CV-19 unvaccinated and those who never submitted to a PCR swab test have been repeatedly found to have contamination/infestation of the blood as well, albeit, to a lesser degree. [14] Unfortunately, because this issue is being actively ignored/suppressed and those who should be scientifically investigating it and attempting to find a cure, have failed to do so, the best that can be obtained is the anecdotal reports of individuals with small numbers of patients.
Evidence of Micro/Nanotech Infestation:
In many respects, the signs [15] and symptoms of MT/NT infestation are the same as “Long COVID” or CV19 vaccine injury. Unfortunately, the list is extremely extensive. It may be that they are all part of the same overall transformation/poisoning of the body that is traceable to the many toxins now known to be contained in CV19 vaccines and many other vaccines and substances. [16] Some of the likely culprits include graphene family nanoparticles (GFN’s), lipid nanoparticles (LNP’s) [17] such as polyethylene glycol (PEG), an assortment of hydrogels (potentially natural and synthetic), aluminum, heavy metals, cesium 137, thulium, polyamide polymers and polyacrylics among others.
Several new phenomena were reported after December 2020 when the CV19 vaccine roll-out commenced, including, 1) Magnetism at the site of injection and in other body locations such as the head, 2) MAC emissions [18] being broadcast from CV19 vaccinated individuals (including corpses in cemeteries), that can be identified using blue tooth technology, so-called 3) Calamari-like “clots” [19] aka rubbery (sometimes, extremely long) intravascular obstructions in arteries and veins that on [mass spec. chemical analysis] [20] do not contain iron, indicating they are not composed of red blood cells, meaning they are not blood clots, 4) Marked increase in excess (unexpected) deaths [21], to name only a few.
The health problems that are associated with taking MT/NT laden CV19 and other injections and internalized through other sources, can be categorized as follows:
Cardiovascular—Myocarditis (inflammation of the heart muscle), Myocardial Infarction (MI or heart attack), CVA (cerebrovascular accident/stroke), PE (pulmonary embolism/clot in pulmonary artery), Peripheral Arterial Occlusion (blood clot in major artery) Arterial Aneurysms.
Neurological—Seizures, Bell’s Palsy, Guillain Barre Syndrome (GBS), Parkinson’s Disease, Creutzfeldt-Jakob Disease, Multiple Sclerosis Flare-Ups, Paralysis, Bain Fog, Loss of Control of Arms or Legs, Paresthesia (burning, numbness, tingling, itching or prickling sensations), Dysesthesia/(chronic pain), Muscle Pain and Weakness.
Immunosuppression and Aggressive Cancer—VAIDS (vaccine acquired immune deficiency syndrome), Turbo Cancer (new, extremely fast growing, where death occurs within weeks or a few months, paradoxically, now being seen in very young people), Recurrent Cancer (after long period of remission, usually more aggressive than original presentation).
Reproductive Dysfunction—Infertility in males and females, Impotence, Pregnancy Loss, Contamination of Breast Milk.
Dermatologic—Blistering, Peeling, Eruptions, Maculo-papular rashes.
Autoimmune Disturbances—Graves’ Disease, Diabetes (new onset and difficulty regulating well-controlled cases), Systemic Lupus Erythematosis, Inflammatory Bowel Disease, Hashimoto’s Thyroiditis, Myasthenia Gravis, Psoriatic Arthritis among many others.
Intellectual/Emotional/Spiritual—Loss of Critical Thinking Skills, Recent Onset of Memory Loss with or without Word-Finding Difficulties, Inability to Concentrate, Depression, Anxiety, Personality Changes, Loss of Connection to God with inability to pray or to meditate on Divine matters.
The above is not intended to be a comprehensive delineation of health problems resulting from taking MT/NT laden CV19 and other injections or substances by any route of administration. It is representative of a constellation of issues now being documented.
The Symptomatic:
It seems from multiple sources of circumstantial evidence, symptomatic persons are made up of the CV19 injected, PCR swab-tested, and to a lesser extent those subject to being shed [22] upon through close proximity to people with a high nanotech burden. It may be that some symptomatic people with no history of CV19 injections, PCR tests or shedding exposure have been contaminated from air, water, food or some other non-vaccine related injection/procedure but these likely constitute relatively few, compared with the total of such cases.
The Asymptomatic:
Asymptomatic persons are those who have no signs or symptoms of anything seemingly referable to nanotech or microtech infestation. Like those in the symptomatic group, they may have other pre-existing medical conditions which arose prior to December 2020 or after, but they would not otherwise suspect that their blood and tissues are contaminated. It is unclear how many people in this group have abnormal blood, which is very unfortunate. If the asymptomatic are relatively free of nanotech infestation, and not in need of remediation/detoxification, it would be a much simpler clinical problem to deal with. Then, countermeasures could be concentrated on the symptomatic (sick and suffering).
How might we answer these questions?
It is important to at least attempt a clinical study, or multiple studies designed to address these timely issues. There are numerous ways in which this might be done. The following discussion outlines some of the parameters that should be considered.
Hypothetical Materials and Methods:
The first step would be to ascertain how much MT/NT/exposure/contamination [23] exists in the general human population, which, admittedly is highly variable for a multiplicity of reasons. A number of studies could be carried out in an attempt to develop a baseline. Unfortunately, there are many mechanisms by which MT/NT exposure/contamination has been achieved. The most obvious is through injection of intentionally tainted products such as vaccines. However, nanoparticulates can be successfully administered through inspired air, food, water and other sources such as oral and trans-dermal medications, supplements and the like. It would be virtually impossible to control for all these variables which is a significant limitation to any such study.
The second step (either sequentially or simultaneously) would be to plan a set of prospective studies designed to determine which treatment modalities [24], either individually or in combination, can achieve objectively verifiable decrease in MT/NT contamination, for example, using live blood analysis (hereinafter LBA) as a metric. The idea would be to use LBA to determine how much MT/NT contamination each enrollee had prior to treatment/remediation/detoxification. At intervals, LBA would be repeated to ascertain what if any effect a given modality achieved in each respective participant.
For step one, where the goal is to ascertain how much MT/NT/exposure/contamination exists in the general population, something like the following might be envisioned:
Ideally, a call would go out, looking for roughly 400 people who would be enrolled in a clinical study, the goal of which would be to check their status using LBA. The idea would be to obtain two roughly equivalent groups, 200 CV19 vaccinated and 200 CV19 unvaccinated people. Each of these would then be further divided into 2 cohorts for a total of 4. The CV19 vaccinated group would contain 2 cohorts made up of those with a history of having undergone PCR swab testing and those who did not. For the purposes of constructing the 4 cohorts, no attempt would be made to determine whether any participant engaged in mask wearing. Similarly, the CV19 unvaccinated group would be comprised of those who underwent PCR swab testing and those who did not. In order to obtain this information, a very detailed medical history form would be completed by each enrollee that includes a list of all vaccines taken and any untoward reactions/complications as well as any PCR tests, including the number of times performed and any and all medications taken, especially concentrating on the period of March 2020 through the date when the blood sample was taken.
Several certified practitioners/technicians would be employed to draw blood and perform a LBA on specimens utilizing an HDMI-LED darkfield [25] capable microscope. The person obtaining the specimen would take it to a close-by isolated location in the same building, so the person doing the live blood analysis would not know anything about the source from which it was obtained. None of the practitioners/technicians would have access to any of the medical history data thus eliminating the possibility of bias being introduced. Detailed photographs and videos would be taken of each LBA specimen along with any notes or comments that were made, after which, all data from each patient [including the slides(s)] would be identified by number and catalogued/stored. Only the study sponsors would have access to the corresponding personal information.
One concern is that unless the study is prospective, it will provide only a snapshot in time, (assuming all participants can have their blood drawn at roughly the same week and immediately following their completion of the detailed personal medical history form).
If the study were to continue prospectively, at six-month intervals for at least one year, more might, theoretically be learned. One caveat however is that some participants might undertake various treatments/remediation strategies subsequent to the first LBA. The only way to avoid these uncontrolled and confounding variables would be for participants to commit to not undergo any treatment/detoxification of MT/NT during the study period. While the lack of solid evidentiary data with respect to treatment protocols at present might make this an ethically acceptable option, it could only be requested and must not be coerced or demanded in any way. If after proper informed consent was sought and given, it might [26] be acceptable to proceed. Some (for example, the asymptomatic) might agree to it. Given enough participants, valuable information may be obtained. Another challenge in carrying the study out prospectively is that the detailed medical history form would need to be updated prior to each additional LBA.
Prior to commencing the baseline study, a decision would need to be made with respect to whether those who have already undertaken treatment/remediation are eligible for inclusion. If enough participants could be obtained who have not done so, it would probably be better not to include those who have. In this way, potentially confounding variables could be minimized.
Lastly, it is unknown how difficult it might be to obtain the participants envisioned.
Possible questions to be answered:
Were symptomatic persons more likely to be CV19-injected or PRC swab tested?
Were asymptomatic persons less likely to be CV19-injected or PRC swab tested?
Were CV19-injected persons more likely to have PCR swab testing done?
Were CV19-uninjected persons less likely to have PCR swab testing done?
Did symptomatic persons have greater micro/nanotech infestation by LBA?
Did asymptomatic persons have lesser micro/nanotech infestation by LBA?
Did the CV19-injected and PCR swab tested cohort have the greatest amount of micro/nanotech infestation by LBA? How do the other 3 cohorts compare? Which cohort has the least?
Was CV19 vaccination status more/less associated with MT/NT infestation (e.g. do those with the most injections have more MT/NT infestation than those with fewer injections)? If so, is the effect progressive and unrelenting?
What percentage of each cohort had frequent/daily exposure to CV19-injected individuals or groups? This is admittedly difficult to answer due to the fact that it is quite subjective.
The first eight above are fairly objective while the last is quite subjective. The most objective are the vaccination status, whether PCR swab testing was done, and the results of lab and imaging tests when available. Symptoms are intermediate between highly objective and very subjective criteria.
One major prediction would be that a much larger percentage in the symptomatic group would have a history of being CV19 vaccinated/boosted, and PCR swab tested as well as greater evidence of micro/nanotech infestation as compared with the asymptomatic group.
It seems appropriate, for multiple reasons, to predict that the CV19 vaccinated/boosted, would have more PCR swab testing done than the CV19 unvaccinated. We know for example that people who have had repeated booster injections have a higher incidence of becoming ill than those who have never been injected with a CV19 vaccine.
Final Thoughts:
Many people rightly express anxiety [27] about whether they should attempt to rid themselves of what they assume is nanotech or microtech infestation in their bodies. The vast majority appear to have no access to qualified [28] practitioners of the live blood analysis technique. Those with the greatest concern are individuals who were subjected to multiple CV19 injections/boosters and or PCR swab tests. An additional unknown number are those who were not CV19 vaccinated, or PCR swabbed, their apprehensions being based on the apparent, progressively increasing contamination in the uninjected. Perhaps worse yet, some in each cadre have no obvious symptoms or signs of MT/NT infestation. Due to a paucity of relevant data, it is difficult to know how to advise those with questions/fears. Particularly so, are totally asymptomatic CV19 unvaccinated/PCR unswabbed persons, unless there is evidence of significant contamination by use of a modality such as LBA. It would be best to know which of the 4 hypothetical cohorts have the most MT/NT infestation and which, the least and so on, as it might assist in triage efforts. It is morally reprehensible that the proper authorities and health agencies have not admitted what is now a horrendous and undeniable global health problem or provided any medical assistance to those who are in desperate need of it.
Hopefully, this essay will help further an exchange of ideas on this vitally important topic. Perhaps some qualified individuals will design and implement one or more clinical studies as alluded to above. As always, readers are strongly encouraged to examine the endnotes carefully and “click” on the links. A great deal of vital information can be found there.
Lastly, a short list of relevant Internet of Bodies (IOB) literature with links is also included. It is clear that part of the reason for the MT/NT contamination/infestation currently underway, is to bring about the internet of bodies which globalists have indicated is part of their plan to enact a [universal internal digital ID/CBDC/social credit (read punishment) score system] [29].
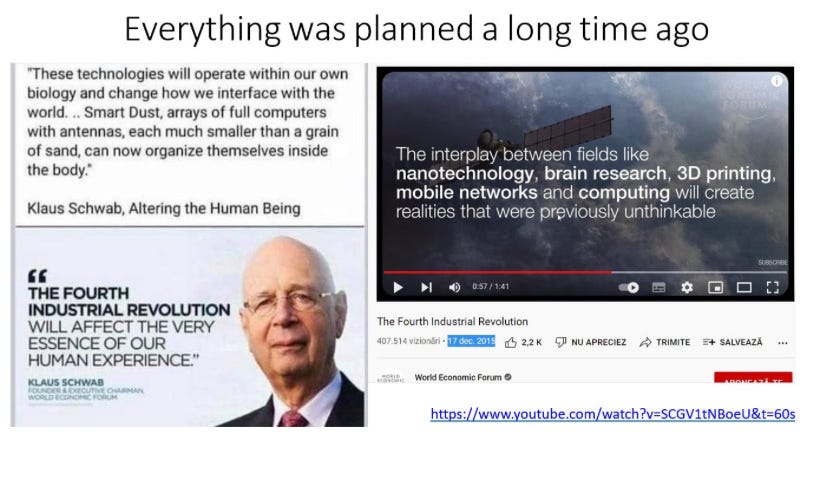
Image courtesy of Dr. Anita Baxas
Related Internet of Bodies Literature:
End Notes:
[1] DETECTION OF GRAPHENE IN COVID19 VACCINES BY MICRO-RAMAN SPECTROSCOPY. This was dated November 2, 2021 but Dr. Campra made his first announcement several months earlier.
[2] Toxicity of graphene-family nanoparticles: a general review of the origins and mechanisms. See also Graphene Oxide Nanosheets Stimulate Ruffling and Shedding of Mammalian Cell Plasma Membranes. Many more could be cited but time and space prohibit a more exhaustive listing.
[3] Graphene oxide induces dose‑dependent lung injury in rats by regulating autophagy.
[4] See for example, What is in the so-called COVID-19 Vaccines? Part 1: Evidence of a Global Crime Against Humanity. International Journal of Vaccine Theory, Practice, and Research 2(2), September 3, 2022. See also: Dr. Robert Young & Science Team Reveal Graphene, Aluminum, Lipid Nanoparticle (LNP) Capsids, Poly-Ethylene Glycol (PEG) & Parasites in Pfizer, Moderna, AstraZeneca & Janssen Vaccines and Diblasi, L. and Sangorrin, (2024). Analysis of COVID-19 Injections — 50 Undeclared Chemical Elements, Graphene Oxide, Fluorescent Particles – Conversation with Biotechnologist Lorean Diblasi. Interview with Ana Maria Mihalcea. If human health had been the motivating factor, even one reproducible finding of graphene contamination should have been enough to ban the products after which an exhaustive investigation should have commenced. After 25 more, there is no other conclusion but that it was inserted for the express purpose of causing harm.
[5] New Quality-Control Investigations on Vaccines: Micro- and Nanocontamination. The authors concluded: “The analyses carried out show that in all samples checked, vaccines contain non biocompatible and bio-persistent foreign bodies which are not declared by the Producers, against which the body reacts in any case.” This study was published in 2017, almost four years before the CV19 injectable products were deployed. What possible excuse is there for not knowing about widespread contamination of all vaccines? What conceivable reason, other than malevolence, is there for why public health authorities and manufacturers refused to acknowledge and rectify this problem?
[6] This was remarkable because two of these products (Pfizer and Moderna) were said to contain mRNA in significant quantities and in others, DNA and proteins. In many instances there was either no nitrogen or phosphorus at all or only trivial amounts, meaning they contained nothing biological.
[7] See this extensive recent study: (PDF) Real-Time Self-Assembly of Stereomicroscopically Visible Artificial Constructions in Incubated Specimens of mRNA Products Mainly from Pfizer and Moderna: A Comprehensive Longitudinal Study (researchgate.net). The reference section of this paper is an outstanding resource.
[8] Geanina Hagimă MD. (2023a). Interview. Electron Microscopy of Comirnaty, Moderna C19 Shots, Dental Anesthetics & Pneumovax.
[9] Nanobots In Covid 19 Unvaccinated Blood Darkfield Live Blood Analysis 4000x Magnification; Nanotechnology and Transhumanism Unfolding Before our Eyes with Dr. Mihalcea - Interview with Laura-Lynn Tyler Thompson; Graphene and Hydrogels Building a Neural Network; Nanotech Turning Us Into Cyborgs Is Real. This is only a small sampling of what is available.
[10] Preliminary Treatment Protocols for The Covid Vaccine Injured: Video, Anita Baxas, MD. A great deal of valuable information is provided with respect to the contents of CV19 “vaccines”, the nature of the MT/NT infestation that has been documented in the blood of virtually all human beings tested to date as well as possible treatment/remediation modalities to consider. At this time there is clearly a great deal more that is unknown than known, (based on what is available in the public domain).
[11] This includes reviewing many articles written by citizen investigators who use microscopy and live blood analysis, among other modalities, to investigate a plethora of injectables, supplements, oral medications and human blood.
[12] In 2022, there appeared to be a significant difference in the blood of CV19 vaccinated as compared with CV19 unvaccinated blood. See: Dark-Field Microscopic Analysis on the Blood of 1006 Symptomatic Persons After Anti-COVID mRNA Injections from Pfizer/BioNtech or Moderna. International Journal of Vaccine Theory, Practice, and Research. Franco Giovannini, MD, Riccardo Benzi Cipelli MD, DDS and Gianpaolo Pisano MD, OHNS 2(2), August 12, 2022. This was one of the earliest, large studies to document that the blood of CV19 vaccinated persons was markedly abnormal as compared with the CV19 unvaccinated. Despite the fact that only 12 had blood samples from before CV19 vaccination, the differences (pre vs.: post injection) were remarkable (the authors reported normal blood in the 12 prior to vaccination). This no longer appears to be the case, and the explanation has not been adequately delineated (in the public record). I have been unable to view the entire manuscript and therefore it is unclear whether the 12 developed symptoms only after vaccination (this is presumed since they had normal blood before) or whether they had symptoms prior to vaccination. It would be wonderful if this group could do the kind of study being discussed here.
[13] People with symptoms of MT/NT infestation, appear on live blood analysis, to have much more evidence of MT/NT infestation. It may not actually be the case however. It could be because not as many asymptomatic people have had a LBA. See two recent reports from Ana Maria Mihalcea MD and Anita Baxas MD respectively: Microrobots And Nanobots Everywhere! Seen In All COVID Unvaccinated Blood Samples Now- Darkfield Live Blood Analysis Samples and Dark Field Microscopy of Jabbed & Unjabbed People and a Steak which add to the circumstantial evidence already compiled by multiple citizen investigators over the past 3 years. There appears to be more MT/NT infestation in the blood of the CV19 unvaccinated than there was 2 years ago.
[14] This is more of a working hypothesis, due to the fact that anecdotal reports of live blood microscopists, with a small number of patients, are all that is available for review at present.
[15] For the purposes of this article, “signs” shall include not only physical findings on patient examination but any relevant lab tests, imaging procedures or other such findings.
[16] Many of these same substances have now been found in food (see for example, Self-Assembling Construction Sites in Fruit and Vegetables and a Chicken), water (see, 10 Brands of Coconut Water also full of Nanos and Primo Water is full of moving Nanobots), nutritional supplements (see. Nano-filled Natural Factors® Supplements from the Muppet Planet Koozebane?), injectable anesthetics such as Lidocaine, Pontocaine, Mepivacaine, Articaine, Marcaine and Prilocaine, (for example, see: Ask your Dentist from 1994 if Nanos Were Right for You! Investigations of Dental Anesthetics under the Microscope Part 6, and Compounded Dental Anaesthetic) and the analysis and statement by Jessica C. Hankins, University of Colorado Boulder Raman Microspectroscopy Laboratory; I can affirm the presence of graphene oxide particles in this anesthetic with high confidence, as well as various medications and air-borne particulates. Therefore, many sources might contribute to the degree of infestation found in each individual as well as their personal history of exposure, individual tolerance and their genetic constitution.
[17] Apparent Cytotoxicity and Intrinsic Cytotoxicity of Lipid Nanomaterials Contained in a COVID-19 mRNA Vaccine. (2023). International Journal of Vaccine Theory, Practice, and Research, 3(1), 957–972.
[18] Dr. Luis Benito detected MAC (Media Access Control) address emissions on his phone when vaccinated patients entered his office. Non-vaccinated patients did not emit any MAC addresses as of three years ago. Also see Blue Tooth Mac Address Phenomenon From Covid 19 Shots -Conversation with Dr. Pedro Chavez -EP 30 (rumble.com) who began seeing patients manifesting the MAC address phenomenon in April, 2021, those in whom magnetism was being discovered at the site of their CV19 injections suggesting that these two phenomena are related. There is a great deal of detailed information contained in that interview. An additional video is, 'BlueTRUTH' Documentary – The “Vaxxed” MAC Address Phenomenon. Dr. Chavez reported on 15 unvaccinated patients. Ten had no MAC address emissions but five did. Of the five with MAC emissions, four had a history of PCR swab testing and one had a history of sexual relations with a CV19 multiply vaccinated individual. It is unclear whether any of the fifteen had symptoms. This is evidence of the Internet of Bodies (IOB) being constructed. See reference list that follows, for details with respect to the IOB. Additional references can be found in the BlueTruth Documentary at the link provided above.
[19] See: British Institute of Embalmers: Results of the July 2024 BIE Blood Clot Survey, and Worldwide Embalmer Blood Clot Surveys, and Results of the People's Blood Clot Survey as of October 1, 2024, both are courtesy of Laura Kasner. In addition, there is the People’s Blood Clot Survey Data pdf with comments.
Also see: Are the Embalmers Clots Occurring in the Living? Whistleblower from a Catheter lab speaks out about observations, a video conducted by Dr. Philip McMillan that documents an extensive array of intra-arterial and intravenous calamari-like “clots” extracted from living patients, best described as rubbery “intravascular casts”, not traditional blood clots. The angiograms and patient specimens are stunning. The whistleblower indicated that these began appearing in the latter half of 2021.
[20] See the elemental analysis performed by Mike Adams and reported on Natural News, 8/17/22, now over 2 years ago. This evidence should be correlated with that documented in number 19, directly above.
[21] Abnormal Clots and All-Cause Mortality During the Pandemic Experiment: Five Doses of COVID-19 Vaccine Are Evidently Lethal to Nearly All Medicare Participants. (2023). International Journal of Vaccine Theory, Practice, and Research, 3(1), 847-890, From the abstract: “The upshot is that 5 doses, on the average, will kill all the Medicare participants who accept the advice of the CDC…It is certain that the injectables are increasing all-cause mortality across the globe…In the dataset from Connecticut, 1.22 persons in 10,000 survived 5 doses during the experimental pandemic in order to take a 6th dose. Those who did so died, on the average, in 34 days. Only 1 participant survived 6 doses to receive a 7th and died within 69 days at the age of 68.” Also see: K.A. Beattie, “The Vaccines Were the ‘COVID-19 Pandemic’: An Update of Beattie’s Worldwide Bayesian Analysis of the Effects of the Experimental COVID-19 Injections on Deaths, Cases, and Excess Mortality in 210 Countries and 38 Regions.” (2024). International Journal of Vaccine Theory, Practice, and Research, TBA.
[22] This should be more fully investigated to see if what is only a presumption, can be verified. Admittedly, doing so might prove to be very challenging. There seems at present, to be circumstantial evidence for it but solid scientific proof in the public domain appears to be lacking. Nevertheless, there are several circumstantial evidentiary reasons why shedding of MT/NT is possible. First, there was no legitimate health-related reason to cite the 70% vaccination threshold as a goal (the injection is not a vaccine, there was no pandemic by traditional standards and no properly isolated virus). The hypothesis is that the perpetrators knew they could effectively reach the entire global population if they could get 70% injected. Second, they made it clear that shedding was a possibility in what we now know were fake CV19 “vaccine” trials (a kind of performance theater). Third, there is anecdotal evidence which seems to support it. I am unaware of any anecdotal evidence against it. Moreover, how many people who have symptoms or MT/NT in their blood on LBA are certain they have not come in contact with vaccinated individuals, (probably very few)? —the negative case is more difficult to prove. Fourth, I know of no medical/physiological reason why MT/NT should be incapable of traveling through the air as people who have it, breathe in an out in their vicinity. GFN’s and other toxic materials have been found in atmospheric particulates; people and animals internalize them from the ambient air through the alveolar-capillary membrane in the lungs. The shedding of MT/NT is therefore assumed, but not proven to be, analogous to the contamination that occurs from the atmosphere.
In a private communication I have learned that a person with whom I am in contact, is unconvinced so far about the possibility of shedding MT/NT from one human being to another. I hope he will comment more fully in this forum.
[23] Live blood analysis (LBA) may currently be the best modality for determining the level of contamination present.
[24] Based on what is currently understood, some of these might include, IV EDTA, IV Plaquex, IV Vitamin C, EBOO, IV Glutathione, IV Methylene Blue, NAC, Chitosan and Sodium Citrate. This list is not intended to be exhaustive.
[25] Darkfield microscopy appears to be the best method for visualizing the smallest structures. Self-assembling nanotech/nanobots as small as ~500nm can be seen using standard darkfield microscopy. Generally speaking, electron microscopy is required for structures less than 500nm. For further details with respect to “enhanced dark field microscopy” and Hyperspectral imaging, see references dealing with Special Applications of Dark Field Microscopy section below. I am indebted to Matt’s Microscopy for bringing this to my attention.
[26] These kinds of ethical questions are usually addressed by institutional review boards in cooperation with the designers of clinical studies, but due to the refusal of the relevant institutions/organizations to cooperate or even admit the existence of MT/NT infestation, it is very unlikely to occur.
[27] Part of this comes from an inability to afford the cost of many suggested treatments such as EBOO, IV EDTA, IV Vitamin C and IV Plaquex for example and from the fact that there is no available, intermediate or long-term follow up of these modalities when used for the purpose of treating MT/NT infestation/contamination. Even short-term follow-up is anecdotal and incomplete. Unfortunately, it appears that the oral forms of these, where available so far, appear to be less effective.
[28] Qualified individuals are those who have become proficient at visualizing not only microtechnology in the millimeter size range but those who are capable of finding structures in the nanometer size range as well. These are persons who have acquired great expertise and invariably have microscopes with superior light, optics and darkfield capability.
[29] See my: Digital ID/CBDC/Social Credit Score is a Massive Human Enslavement Program. It is also known that graphene oxide has a “high potential for transmitting signals at gigahertz ranges.”, which makes it an ideal candidate for bringing about the IOB technology integral to the ID/CBDC/SCS (mark of the beast) system. See Radio-frequency characteristics of graphene oxide.
References dealing with Special Applications of Dark Field Microscopy:
Smartphone analysis and dark-field microscopy observation for aflatoxin B1 detection based on the disintegration of core-shell Ag@Au nanoparticles. 2024, Food Bioscience.
“There is a set of important limitations in the conventional microscopies, however. Optical microscopy is unable to detect nanoscale particles (particles having dimensions less than 200 nm) due to its diffraction-limited resolution… Dark-field microscopy is a microscopy technique based on the indirect sample illumination, when the light-focusing condenser is equipped with a circular opaque light stop preventing the direct illumination of the specimen (Davidson and Abramowitz, 2002). Unlike in bright-field illumination, where the specimen is illuminated by a directly focused light producing dark images on white background, in dark-field microscopy only peripheral light illuminates the specimen while the direct light is cut… A particular subtype of optical microscopy, namely (enhanced) dark-field microscopy, offers a great potential for fast, effective, cheap and non-destructive imaging of a range on nanosized materials (Roth et al., 2015a)… In recent years, the so-called ‘enhanced dark field’ microscopy, based on using higher numerical aperture light condensers and variable numerical aperture objectives has emerged, which allows for imaging of nanoscale particles (starting from 5 nm nanospheres) using almost conventional optical microscopy methodology. Hyperspectral imaging can turn a dark-field optical microscope into a powerful chemical characterization tool.”
")